Breathing Counter
Count your child's breathing rate in real time using a simple tap-based tool. Designed for use while your child is calm or sleeping.
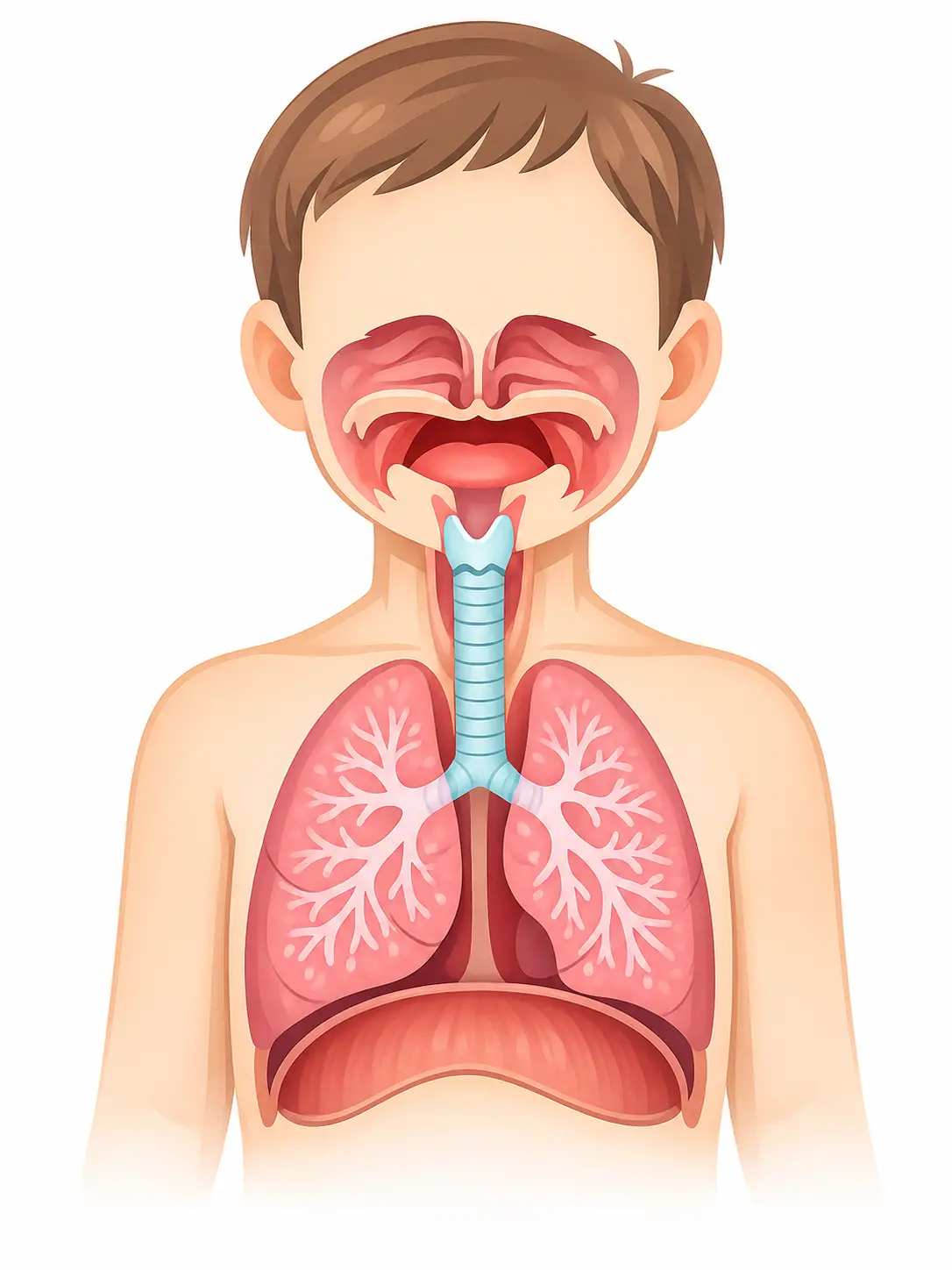
Open Breathing CounterWatching your baby or child breathe and noticing something that does not look right can be frightening. This page is a broad overview of the most common breathing signs parents notice — what they look like, why they happen, and when they need attention. Each symptom links to a more detailed guide.
Tap any card to learn what it looks like, what it sounds like, and how to describe it.

Skin between or below the ribs tugs inward with each breath

Skin at the base of the throat dips inward with each breath
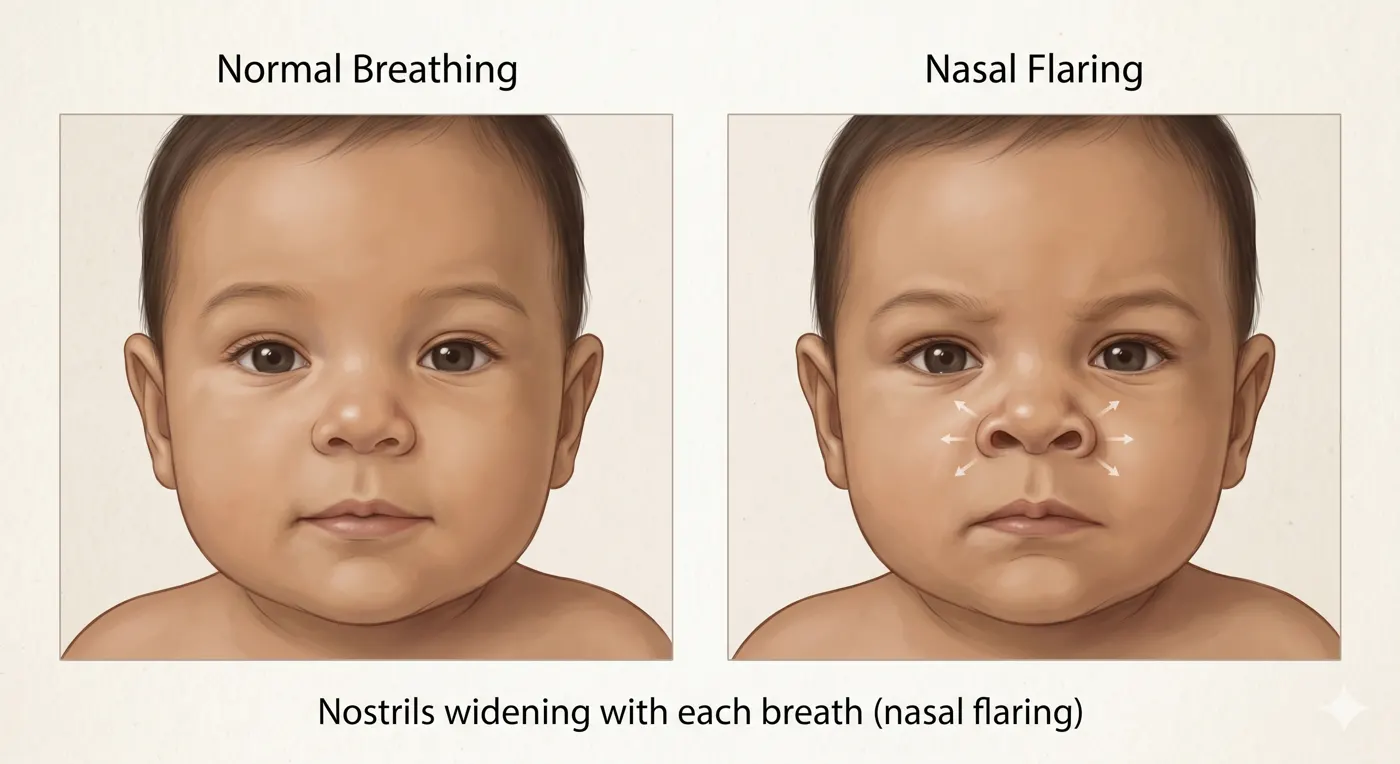
Nostrils spread open wider with each breath in
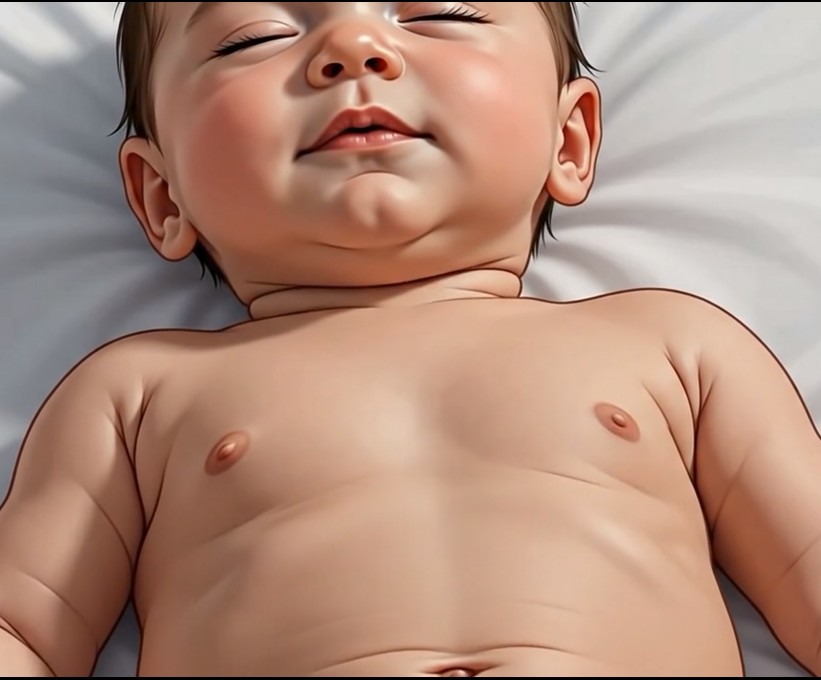
Belly pumping fast and hard with each breath

A harsh squeaky sound when breathing in (stridor)

A short low sound at the end of each breath out

A high-pitched whistling sound when breathing out

A harsh barking cough that sounds like a seal or dog (croup)

Breathing rate consistently above normal for the child's age

Baby stops breathing for a few seconds then starts again

Blue or gray color around the lips, tongue, or fingernails
Count your child's breathing rate in real time using a simple tap-based tool. Designed for use while your child is calm or sleeping.
Open Breathing CounterCreate a clear summary of your child's symptoms to share with another caregiver or at a doctor's visit.
Open Caregiver Handoff


Get pediatrician-designed visual guides and tools like this one, free in the PediaPulse app.
Download PediaPulse Parent →Free · No email requiredNot ready to download?
Get the free guide instead — 5 Baby Symptoms Every Parent Should Never Ignore.
Get the Free Guide →